Login



www.reeleak.com
Reeleak is an alternative to LiveGore, now you can surf and watch LiveGore content directly from Reeleak.
WARNING: UNCENSORED NEWS!
LiveGore is a reality news website which reports on real life events which are of the interest to the public. Includes videos relating to true crime that have been taken from across the world. Due to the graphic nature of materials found on Live Gore, access is restricted to adults only(18+). !!Please leave this website if you under that age!!Important Update!
Please join our telegram channel to get important updates related to this website.
Join now : https://t.me/+aI6AdrheUSlhYTNh/
New poll : https://t.me/c/2146536856/5/
New note : https://t.me/c/2146536856/7/
Join our telegram for news update!
https://t.me/+aI6AdrheUSlhYTNh/
Announcement Box
Please check our new announcement.
READ : https://t.me/livegoredotcom/37
ARE YOU OVER 18 YEARS OLD?
You must be 18 or older to enter this website.
By clicking "YES", you confirm that you are of legal age to view this content.
If you are under 18, please click "NO" to exit the site.
Fig 1: Extent of the decubitus ulcer is shown. Posterior pelvis and femur are exposed in the base of the wound. The small contralateral decubitus ulcer was treated successfully with local wound care.
Fig 2: Mid-shank guillotine amputation followed by removal of the remaining tibia and fibula and disarticulation of the femur.
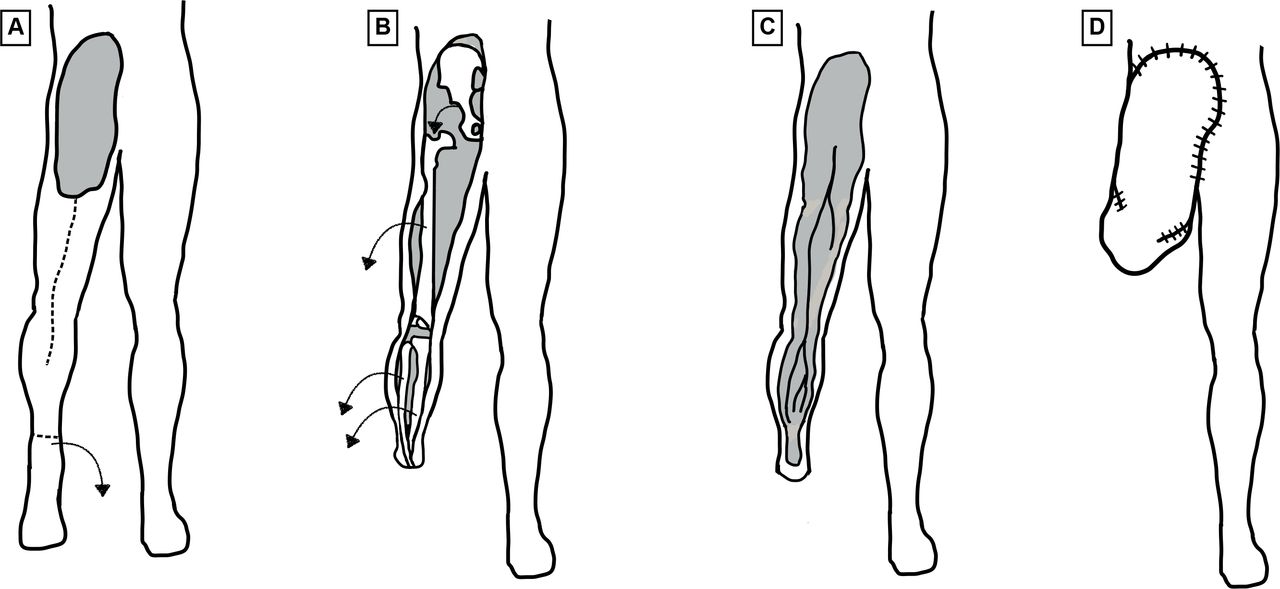
Fig 3: A step-by-step drawing of the surgical process. (A) Incision from the gluteal cleft to popliteal fossa and guillotine distal shank amputation. (B) Sever all knee ligaments. Remove the tibia and fibula. Remove femur after distal mobilization and disarticulate hip posteriorly through the decubitus ulcer. (C) Define vascular anatomy to avoid injury. (D) The folded newly created final flap. Created by approximating the skin of the most distal portion of the flap (the mid-shank) to the superior most aspect of the sacral decubitus ulcer and suturing laterally and medially flap to pelvis, then flap to flap to close the wound.
Fig 4: The mature flap several months postoperatively.
We accepted a transfer of a paraplegic female with spina bifida aged 34 years who presented to an outside hospital with left-sided sacropelvic and femoral osteomyelitis resulting from very large pressure ulcers (figure 1). Following initial debridement of the ulcers, she became acutely ill. Plastic surgery, orthopedics, and acute care surgery all recommended a palliative care consult. Her parents came to us for a second opinion. On arrival, we found the patient to be septic, obtunded, malnourished, and in renal failure. For acute management, she was intubated, resuscitated, and initiated on broad-spectrum antibiotics. She was then taken to the operating room (OR) where her wound was thoroughly explored and debrided, and antibiotics were tailored to her cultures. She responded well to initial management, regained renal function, and was successfully weaned off the ventilator. As she was lucid, she was included in a conversation about possible wound management options.
Once she was stabilized from an infectious perspective, which included an end sigmoid colostomy to optimize wound care, we established nasoduodenal nutrition with the goal of giving her 2 g/kg of protein per day. We then had a long discussion with the patient, her family, and the plastic surgery team before concluding that if we did not achieve coverage of her wound and give her a durable, well-vascularized weight-bearing surface, any attempt at closure would ultimately fail. In this context, particularly given the fact that she did not use her legs, we agreed that the least complex operation with the greatest chance of long-term success was a fillet of leg flap.
We proceeded to the OR the next day with our plastic surgery colleagues on standby in case we were unsuccessful, and she required another solution. As her ulcer was quite large, it afforded easy access to her pelvis and femur. To create our flap, we made an incision from the gluteal cleft to popliteal fossa, dissected out and preserved the popliteal complex, and performed a mid-shank guillotine amputation. Next, we severed all knee ligaments, removed the tibia and fibula from the shank, disarticulated the left femur from the pelvis, and deboned the femur from the thigh (figure 2). This process resulted in the appropriately named ‘fillet of leg’ flap. The flap was folded, approximating the skin of the most distal portion of the flap (the mid-shank) to the superior most aspect of the sacral decubitus ulcer. We sutured laterally and medially flap to pelvis, then flap to flap to close the wound. Figure 3 shows a step-by-step line drawing of this process.
The patient recovered in the hospital for 2 weeks, followed by 4 weeks in subacute rehabilitation. She made a full recovery with her mature flap shown in figure 4. She has not had recurrence of any ulcers and has resumed working from home.
From the surgeon’s perspective, the fillet of leg flap offers ample bulk unlike a myocutaneous or perforator-based flap, does not require a vascular anastomosis, provides versatility in coverage and surface area of wound type, and does not require ligation of the aorta, vena cava, or thecal sac as in a hemicorporectomy. This flap also reduces donor site morbidity by repurposing lower extremity tissue that is available and not otherwise used and can result in improved functional outcomes allowing resumption of activities of daily living and wheelchair use.
Ultimately, the fillet of leg flap is a good flap for a bad problem.
Important!
Your post might be deleted/hidden when other users reported/flag it. Think twice with your post title/description/comments, because the content is automatically deleted/hidden by the system. If you need quick action to delete any content in this website, you can click the Report content! button below.
We apologize for the flagged problem encountered, but for your information, every post that is flagged will be assessed as to whether it needs to be deleted or published again, this is to avoid uploading prohibited content. For that, every hidden media will be published again if it does not violate the rules of this site. In addition, posts that are uploaded repeatedly will also be deleted. We would like to emphasize that if your account is found to continue flagging and down-voting posts for no reason, your account will be blocked by the system. If you think the system has mistakenly blocked your account, you can ask us to unblock your account, but it depends on the logs we check based on the mistake you made. We try to be fair to all users, so action must be taken. Any problem can directly contact us through the Feedback form. Thank you for understanding.
- Moderator